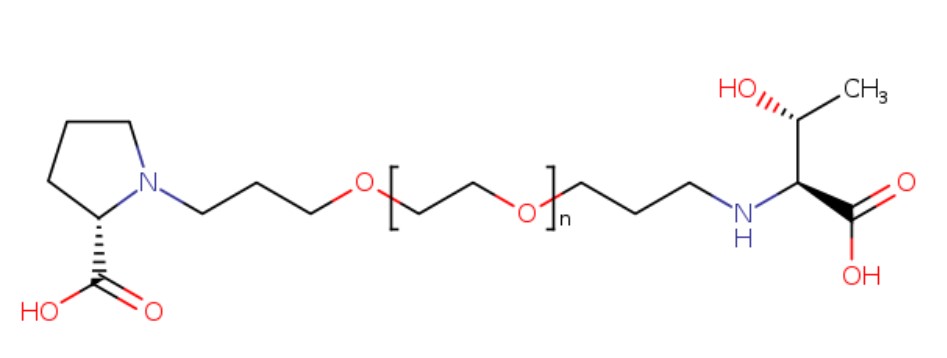
Poly(oxy-1,2-ethanediyl), α-hydro-ω-hydroxy-, 1-ether with immunoglobulin G4 [1-[1-(3-hydroxypropyl)proline]] (human Fc fragment), (3→3′)–disulfide with immunoglobulin G4 (human Fc fragment), 1′′-ether with granulocyte colony-stimulating factor [N–(3-hydroxypropyl),17-serine,65-serine] (human) (ACI)
A long-acting, recombinant analog of the endogenous human granulocyte colony-stimulating factor (G-CSF) with hematopoietic activity. Similar to G-CSF, eflapegrastim binds to and activates specific cell surface receptors and stimulates neutrophil progenitor proliferation and differentiation, as well as selected neutrophil functions. Therefore, this agent may decrease the duration and incidence of chemotherapy-induced neutropenia. Eflapegrastim extends the half-life of G-CSF, allowing for administration once every 3 weeks.
A long-acting GCSF that consists of 17th serine-G-CSF conjugated to the G4 fragment HMC001 via a PEG linker.
Neutropenia is a relatively common disorder most often due to chemotherapy treatments, adverse drug reactions, or autoimmune disorders. Chemotherapy-induced neutropenia is a common toxicity caused by the administration of anticancer drugs. It is associated with life-threatening infections and may alter the chemotherapy schedule, thus impacting on early and long term outcome. Febrile Neutropenia (FN) is a major dose-limiting toxicity of myelosuppressive chemotherapy regimens such as docetaxel, doxorubicin, cyclophosphamide (TAC); dose-dense doxorubicin plus cyclophosphamide (AC), with or without subsequent weekly or semiweekly paclitaxel; and docetaxel plus cyclophosphamide (TC). It usually leads to prolonged hospitalization, intravenous administration of broad-spectrum antibiotics, and is often associated with significant morbidity and mortality.
Current therapeutic modalities employ granulocyte colony-stimulating factor (G-CSF) and/or antibiotic agents to combat this condition. G-CSF or its other polypeptide derivatives are easy to denature or easily de-composed by proteolytic enzymes in blood to be readily removed through the kidney or liver. Therefore, to maintain the blood concentration and titer of the G-CSF containing drugs, it is necessary to frequently administer the protein drug to patients, which causes excessive suffering in patients. To solve such problems, G-CSF was chemically attached to polymers having a high solubility such as polyethylene glycol (“PEG”), thereby increasing its blood stability and maintaining suitable blood concentration for a longer time.
Filgrastim, tbo-filgrastim, and pegfilgrastim are G-CSFs currently approved by the US Food and Drug Administration (FDA) for the prevention of chemotherapy-induced neutropenia, While the European guidelines also include lenograstim as a recommended G-CSF in solid tumors and non-myeloid malignancies, it is not approved for use in the US. Binding of PEG to G-CSF, even though may increase blood stability, does dramatically reduce the titer needed for optimal physiologic effect. Thus there is a need to address this shortcoming in the art.
Eflapegrastim, as known as Rolontis ®, SPI-2012, HM10460A, and 17,65S-G-CSF, is a long-acting granulocyte-colony stimulating factor (G-CSF) that has been developed to reduce the severity and duration of severe neutropenia, as well as complications of neutropenia, associated with the use of myelosuppressive anti-cancer drugs or radiotherapy. Eflapegrastim consists of a recombinant human G-CSF analog (ef-G-CSF) and a recombinant fragment of the Fc region of human immunoglobulin G4 (IgG4), linked by a Bifunctional polyethylene glycol linker. In certain embodiments, the recombinant human G-CSF analog (ef-G-CSF) varies from human G-CSF (SED ID NO: 1) at positions 17 and 65 which are substituted with serine (SED ID NO: 2). Without wishing to be bound by theory, it is believed that the Fc region of human IgG4 increases the serum half-life of ef-G-CSF.
[55]
ef-G-CSF is produced by transformed E. coli in soluble form in the periplasmic space. Separately, the Fc fragment is produced in transformed E. coli as an inclusion body. The ef-G-CSF and the Fc fragment are independently isolated and purified through successive purification steps. The purified ef-G-CSF (SEQ ID NO: 2) and Fc fragment (SEQ ID NOs: 3 and 4) are then linked via a 3.4 kDa PEG molecule that was designed with reactive groups at both ends. Eflapegrastim itself is the molecule resulting from the PEG linker binding at each of the N-termini of ef-G-CSF and the Fc fragment. The G-CSF analog is conjugated to the 3.4 kDa polyethylene glycol analogue with propyl aldehyde end groups at both ends, (OHCCH 2CH 2(OCH 2CH 2) nOCH 2CH 2CHO) at the nitrogen atom of its N-terminal Thr residue via reductive amination to form a covalent bond. The resulting G-CSF-PEG complex is then linked to the N-terminal Pro at the nitrogen of the recombinant Fc fragment variant produced in E. coli via reductive amination to yield the final conjugate of Eflapegrastim.
[56]
Example 1: Preparation of Eflapegrastim ( 17,65S-G-CSF-PEG-Fc)
[120]
Step 1: Preparation of Immunoglobulin Fc Fragment Using Immunoglobulin
[121]
Preparation of an immunoglobulin Fc fragment was prepared as follows.
[122]
200 mg of 150-kDa immunoglobulin G (IgG) (Green Cross, Korea) dissolved in 10 mM phosphate buffer was treated with 2 mg of a proteolytic enzyme, papain (Sigma) at 37℃ for 2 hrs with gentle agitation.
[123]
After the enzyme reaction, the immunoglobulin Fc fragment regenerated thus was subjected to chromatography for purification using sequentially a Superdex column, a protein A column and a cation exchange column. In detail, the reaction solution was loaded onto a Superdex 200 column (Pharmacia) equilibrated with 10 mM sodium phosphate buffer (PBS, pH 7.3), and the column was eluted with the same buffer at a flow rate of 1 ml/min. Unreacted immunoglobulin molecules (IgG) and F(ab’)2, which had a relatively high molecular weight compared to the immunoglobulin Fc fragment, were removed using their property of being eluted earlier than the Ig Fc fragment. Fab fragments having a molecular weight similar to the Ig Fc fragment were eliminated by protein A column chromatography (FIGURE 1). The resulting fractions containing the Ig Fc fragment eluted from the Superdex 200 column were loaded at a flow rate of 5 ml/min onto a protein A column (Pharmacia) equilibrated with 20 mM phosphate buffer (pH 7.0), and the column was washed with the same buffer to remove proteins unbound to the column. Then, the protein A column was eluted with 100 mM sodium citrate buffer (pH 3.0) to obtain highly pure immunoglobulin Fc fragment. The Fc fractions collected from the protein A column were finally purified using a cation exchange column (polyCAT, PolyLC Company), wherein this column loaded with the Fc fractions was eluted with a linear gradient of 0.15-0.4 M NaCl in 10 mM acetate buffer (pH 4.5), thus providing highly pure Fc fractions. The highly pure Fc fractions were analyzed by 12% SDS-PAGE (lane 2 in FIGURE 2).
[124]
Step 2: Preparation of 17,65S-G-CSF-PEG Complex
[125]
3.4-kDa polyethylene glycol having an aldehyde reactive group at both ends, ALD-PEG-ALD (Shearwater), was mixed with human granulocyte colony stimulating factor ( 17,65S-G-CSF, MW: 18.6 kDa) dissolved in 100 mM phosphate buffer in an amount of 5 mg/ml at a 17,65S-G-CSF: PEG molar ratio of 1:5. To this mixture, a reducing agent, sodium cyanoborohydride (NaCNBH 3, Sigma), was added at a final concentration of 20 mM and was allowed to react at 4℃ for 3 hrs with gentle agitation to allow PEG to link to the amino terminal end of 17,65S-G-CSF. To obtain a 1:1 complex of PEG and 17,65S-G-CSF, the reaction mixture was subjected to size exclusion chromatography using a Superdex R column (Pharmacia). The 17,65S-G-CSF-PEG complex was eluted from the column using 10 mM potassium phosphate buffer (pH 6.0) as an elution buffer, and 17,65S-G-CSF not linked to PEG, unreacted PEG and dimer byproducts where PEG was linked to 17,65S-G-CSF molecules were removed. The purified 17,65S-G-CSF-PEG complex was concentrated to 5 mg/ml. Through this experiment, the optimal reaction molar ratio for 17,65S-G-CSF to PEG, providing the highest reactivity and generating the smallest amount of byproducts such as dimers, was found to be 1:5.
[126]
Step 3: Preparation of the 17,65S-G-CSF-PEG-Fc Conjugate
[127]
To link the 17,65S-G-CSF-PEG complex purified in the above step 2 to the N-terminus of an immunoglobulin Fc fragment, the immunoglobulin Fc fragment (about 53 kDa) prepared in Step 1 was dissolved in 10 mM phosphate buffer and mixed with the 17,65S-G-CSF-PEG complex at an 17,65S-G-CSF-PEG complex:Fc molar ratio of 1:1, 1:2, 1:4 and 1:8. After the phosphate buffer concentration of the reaction solution was adjusted to 100 mM, a reducing agent, NaCNBH 3, was added to the reaction solution at a final concentration of 20 mM and was allowed to react at 4℃ for 20 hrs with gentle agitation. Through this experiment, the optimal reaction molar ratio for 17,65S-G-CSF-PEG complex to Fc, providing the highest reactivity and generating the fewest byproducts such as dimers, was found to be 1:2.
[128]
Step 4: Isolation and Purification of the G-CSF-PEG-Fc Conjugate
[129]
After the reaction of the above step 3, the reaction mixture was subjected to Superdex size exclusion chromatography so as to eliminate unreacted substances and byproducts and purify the 17,65S-G-CSF-PEG-Fc protein conjugate produced. After the reaction mixture was concentrated and loaded onto a Superdex column, 10 mM phosphate buffer (pH 7.3) was passed through the column at a flow rate of 2.5 ml/min to remove unbound Fc and unreacted substances, followed by column elution to collect 17,65S-G-CSF-PEG-Fc protein conjugate fractions. Since the collected 17,65S-G-CSF-PEG-Fc protein conjugate fractions contained a small amount of impurities, unreacted Fc and interferon alpha dimers, cation exchange chromatography was carried out to remove the impurities. The 17,65S-G-CSF-PEG-Fc protein conjugate fractions were loaded onto a PolyCAT LP column (PolyLC) equilibrated with 10 mM sodium acetate (pH 4.5), and the column was eluted with a linear gradient of 0-0.5 M NaCl in 10 mM sodium acetate buffer (pH 4.5) using 1 M NaCl. Finally, the 17,65S-G-CSF-PEG-Fc protein conjugate was purified using an anion exchange column. The 17,65S-G-CSF-PEG-Fc protein conjugate fractions were loaded onto a PolyWAX LP column (PolyLC) equilibrated with 10 mM Tris-HCl (pH 7.5), and the column was then eluted with a linear gradient of 0-0.3 M NaCl in 10 mM Tris-HCl (pH 7.5) using 1 M NaCl, thus isolating the 17,65S-G-CSF-PEG-Fc protein conjugate in a highly pure form.
[130]
[131]
Example 2: Efficacy Study of Eflapegrastim by Different Dosing Regimens in Rats with Docetaxel/Cyclophosphamide induced Neutropenia
[132]
The efficacy of Eflapegrastim (HM10460A), a long acting G-CSF analogue, was compared with Pegfilgrastim by different dosing regimens in a chemotherapy-induced neutropenic rat model.
[133]
In the following study, the Eflapegrastim was created essentially as described in Example 1.
[134]
(i) Materials for Study
[135]
[Table 1] Test Articles
Name
Batch/Lot No.
Storage Condition
Purity (%)
Expiration Date
Supplier
HM10460A
906617001
2~8 ℃
RP-HPLC: 98.6% IE-HPLC: 97.4%
SE-HPLC: 98.6%
01/31/2019
–
Pegfilgrastim
1070334
2~8 ℃
–
–
Amgen
[136]
[Table 2] Vehicles
Name
Composition
Storage Condition
Supplier
Dulbecco’s phosphate buffered saline (DPBS)
–
2~8 ℃
Sigma-Aldrich
[137]
[Table 3] Neutropenia-Inducing Agents
Name
Batch/Lot No.
Storage Condition
Purity (%)
Expiration Date
Supplier
Cyclo-phosphamide
C3250000
2~8 ℃
–
–
Sigma-Aldrich
Docetaxel
17006
RT (20 – 25 ℃)
–
10/31/2020
Hanmi Pharmaceutical Co.
[138]
Preparing HM10460A Solutions for Subcutaneous Administration
[139]
Preparation of a 61.8 ㎍/kg HM10460A solution for subcutaneous administration: a stock solution of HM10460A (6.0 mg/mL) 92.7 μL was diluted with DPBS 17907.3 μL.
[140]
Preparation of a 372.0 ㎍/kg HM10460A solution for subcutaneous administration: a stock solution of HM10460A (6.0 mg/mL) 558.0 μL was diluted with DPBS 17442.0 μL.
[141]
Preparation of a 496.0 ㎍/kg HM10460A solution for subcutaneous administration: a stock solution of HM10460A (6.0 mg/mL) 744.0μL was diluted with DPBS 17256.0 μL.
[142]
The test article was prepared based on G-CSF protein dosage on drug label(HM10460A.)
[143]
The HM10460A solution for subcutaneous administration was then diluted with DPBS to a final dose concentration of 2 mL/kg.
[144]
Preparing Pegfilgrastim Solutions for Subcutaneous Administration
[145]
Preparation of a 103.3 ㎍/kg Pegfilgrastim solution for subcutaneous administration: a stock solution of Pegfilgrastim (10 mg/mL) 93.0 μL was diluted with DPBS 17907.0 μL.
[146]
Preparation of a 620.0 ㎍/k Pegfilgrastim solution for subcutaneous administration: a stock solution of Pegfilgrastim (10 mg/mL) 558.0 μL was diluted with DPBS 17442.0 μL.
[147]
The Pegfilgrastim solution for subcutaneous administration was then diluted with DPBS to a final dose concentration of 2 mL/kg.
[148]
Preparing Solutions of Neutropenia-Inducing Agents
[149]
To induce neutropenia in rats, Docetaxel/cyclophosphamide was administered using a 1/3 human equivalent dose (Docetaxel 4 mg/kg and CPA 32 mg/kg) (“TC”).
[150]
Preparation of a 32 mg/kg cyclophosphamide solution for subcutaneous administration: cyclophosphamide powder (CPA, Sigma, USA) 2560.0 g was diluted with distilled water (DW, Daihan, Korea) 80000.0 μL.
[151]
Preparation of a 4 mg/kg docetaxel solution for subcutaneous administration: Docel inj. (Hanmi Pharmaceutical, Korea) (42.68 mg/mL) 29070.0 μL was diluted with a commercial formulation buffer (FB, Etahnol 127.4mg/mL in DW) 30930.0 μL.
[152]
The docetaxel and cyclophosphamide solutions for subcutaneous administration were then diluted with FB to a final dose concentration of 1 mL/kg. HM10460A and Pegfilgrastim were diluted with DPBS to a final dose concentration of 2 mL/kg.
[153]
(ii) Methods
[154]
Test System
[155]
[Table 4]
Species and Strain
Rats
Crl: CD Sprague Dawley (SD)
Justification for Species
SD rats were chosen due to their extensive characterization collected from various preclinical studies, especially with the study done to test G-CSF analogue1), 2).
Supplier
Orient Bio corp. Korea 143-1, Sangdaewondong, Jungwon-gu, Seongnam-si, Gyeonggi-do, Korea
Number of animals
Male 125 (at group allocation)
Age
8 weeks (at group allocation)
Body weight range
239.54 ~ 316.46 g (at start of dosing)
Neutropenia induction with chemotherapy
Normal SD rats were administered with Docetaxel 4 mg/kg and CPA 32 mg/kg once intraperitoneally to induce neutropenia. Docetaxel and CPA were injected to induce neutropenia in a rat model according to 4 different regimens: Concomitant (G2-G7), 2 hour (G8-G13), 5 hour (G14-G19), and 24 hour (G20-G25) prior to test article administration.
[156]
Animal Care and Identification
/////////
AS ON DEC2021 3,491,869 VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
Neutropenia in Breast Cancer: Spectrum Pharmaceuticals has submitted an updated regulatory submission to the US FDA for its biologic Rolontis
10/25/2019 Spectrum Pharmaceutical announced that it has filed an updated Biologics License Application (BLA) with the US Food and Drug Administration (FDA) for Rolontis (eflapegrastim).
The BLA for Rolontis is supported by data from two identically designed Phase 3 clinical trials – ADVANCE and RECOVER – that evaluated the safety and efficacy of eflapegrastim in 643 patients with early breast cancer for the treatment of neutropenia with myelosuppressive chemotherapy.
In both studies, eflapegrastim demonstrated the pre-specified hypothesis of non-inferiority (NI) in Duration of Severe Neutropenia (DSN) and a similar safety profile to pegfilgrastim .
Eflapegrastim was approved for medical use in the United States in September 2022.[1][3][4]
Medical uses
Eflapegrastim is indicated to decrease the incidence of infection, as manifested by febrile neutropenia, in adults with non-myeloid malignancies receiving myelosuppressive anti-cancer drugs associated with clinically significant incidence of febrile neutropenia.[1]
Its efficacy has been shown to be non-inferior to pegfilgrastim.[1]
“Eflapegrastim”. Drug Information Portal. U.S. National Library of Medicine.
Clinical trial number NCT02643420 for “SPI-2012 vs Pegfilgrastim in the Management of Neutropenia in Participants With Breast Cancer With Docetaxel and Cyclophosphamide (ADVANCE) (ADVANCE)” at ClinicalTrials.gov
Clinical trial number NCT02953340 for “SPI-2012 vs Pegfilgrastim in Management of Neutropenia in Breast Cancer Participants With Docetaxel and Cyclophosphamide” at ClinicalTrials.gov